Intestinal Obstruction (Paediatric)
Definition :
Bowel obstruction (or intestinal obstruction) is a mechanical or functional obstruction of the intestines, preventing the normal transit of the products of digestion. It can occur at any level distal to the duodenum of the small intestine and is a medical emergency.
Incidence and Etiology:
- Intestinal obstruction occurs in about 1 in 1500 live births.
- Congenital obstructive lesions of the intestines can be viewed as intrinsic (atresia, stenosis, meconium ileus , aganglionic megacolon) or extrinsic (malrotation, constricting bands, intra-abdominal hernias).

Causes of small bowel obstruction include the following:
- Adhesions from previous surgery
- Hernias containing bowel
- Crohn's Disease
- Neoplasms
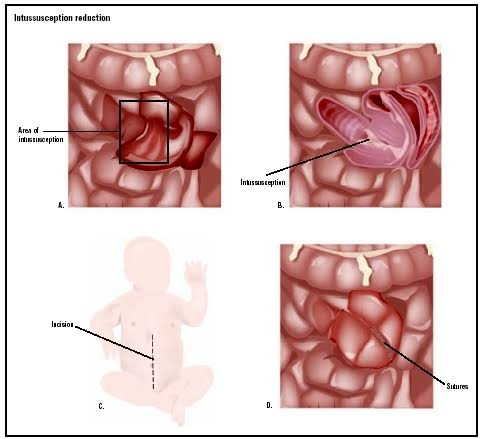
- Intussusception
- Volvulus
- Ischemic Strictures
- Foreign Bodies
- Intestinal Atresia


Causes of large bowel obstruction include the following:
- Neoplasms
- Hernias
- Inflammatory bowel disease
- Colonic volvulus
- Adhesions
- Constipation
- Fecal impaction
- Fecaloma
- Colon atresia
- Intestinal pseudo-obstruction
- Benign strictures (diverticular disease)
- Endometriosis

The normal bowel contains gas and chyme, which is a mixture of food and salivary, gastric, biliary, pancreatic and intestinal secretions. Chyme continues to accumulate even without oral intake. Intrinsic or extrinsic blockage of the small bowel leads to accumulation of secretions that dilate the intestine proximal to the obstruction.
Increased peristaltic contractions and intraluminal pressure may cause frequent loose stools🚽; flatus and vomiting 🤮. The characteristics of stools can suggest the level of obstruction. Intestinal absorption and lymphatic drainage decrease if intraluminal pressure exceeds capillary and venous pressure in the bowel wall.
The bowel becomes ischemic when capillary blood flow stops, allowing bacteria to pass into the peritoneum and then into the bloodstream, leading to septicemia.
Perforation can develop as the ischemia leads to bowel necrosis. Firstly, lymphatic obstruction occurs because of the lesser pressure in these vessels. This is followed by venous obstruction, which accelerates the oedema because blood enters the affected bowel segment but does not have any drainage route. Finally the continuous increase in bowel wall pressure blocks the arterial vessels, leading to ischemic necrosis and perforation. Massive third spacing of fluids rapidly leads to shock , contributing to morbidity and mortality.
Clinical Features:
Depending on the level of obstruction, bowel obstruction can present with the following features:
- Abdominal pain
- Abdominal distension
- Vomiting 🤮 ( biliary or fecal )
- Constipation
- Dehydration and electrolyte abnormalities due to 🤮 vomiting
- Respiratory compromise due to pressure on the diaphragm by a distended abdomen or aspiration of vomitus
- Bowel ischemia or perforation from prolonged distension or pressure from a foreign body
- In small bowel obstruction the pain tends to be colicky (cramping and intermittent) in nature, with spasms lasting a few minutes. The pain tends to be central and mid-abdominal. 🤮 Vomiting occurs before constipation
- In large bowel obstruction the pain is felt lower in the abdomen and the spasms last longer. Constipation occurs earlier and vomiting 🤮 may be less prominent
- Proximal obstruction of the large bowel may present as small bowel obstruction
Signs and symptoms of bowel obstruction, especially in newborns , may be subtle. The following laboratory tests may be useful in diagnosis of obstruction:
1. Blood investigation like:
- Serum electrolyte level
- Blood Urea Nitrogen (BUN)
- Creatinine level
- Glucose level
- Complete blood count (CBC)
- Arterial Blood Gas (ABG) level

3. Stool for occult blood

4. Imaging studies- A flat decubitus and upright radiographs of the abdomen are taken. Radiographic findings include signs of dilated small - bowel loops and air - fluid levels produced by the layering of air and intestinal content. Absence of colonic or rectal gas also indicates a complete bowel obstruction
The pattern of bowel gas on plain radiography can help to differentiate between proximal and distal bowel obstruction
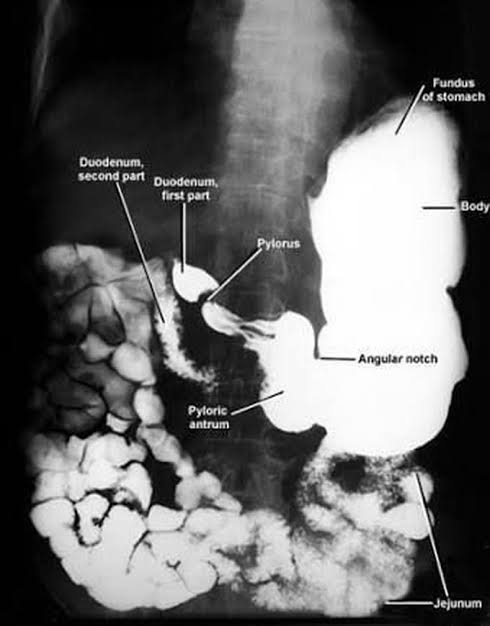
Contrast studies like barium meal and contrast enemas can help to determine the location of obstruction. Contrast studies also reveal whether the obstruction is intrinsic or extrinsic to the bowel
5. Abdominal computed tomography scan: helps to identify causes of chronic partial obstruction, as well as abscess, tumors and other causes of acute abdominal pain
6. Ultrasonography: reveals many intestinal abnormalities, including tumors, mesenteric cysts, and intussusceptions.

Management:
Medical Management:
Medical management of small - bowel obstruction includes the following:
- Stabilize the patient and monitor vital signs
- Replace fluids with diligent intravenous (IV) resuscitation, using isotonic sodium chloride solution or lactated ringer solution
- Opioid pain relievers may be used for patients with severe pain
- Anti-emetics may be administered if the patient is 🤮 Vomiting
- Early bowel decompression with a nasogastric tube decreases the chance of abdominal distension, vomitus and aspiration
- Administer broad - spectrum antibiotics when necrosis or perforation is suspected. Patients who do not respond to non- operative treatment within 12- 24 hrs requires surgical treatment


Comments
Post a Comment